


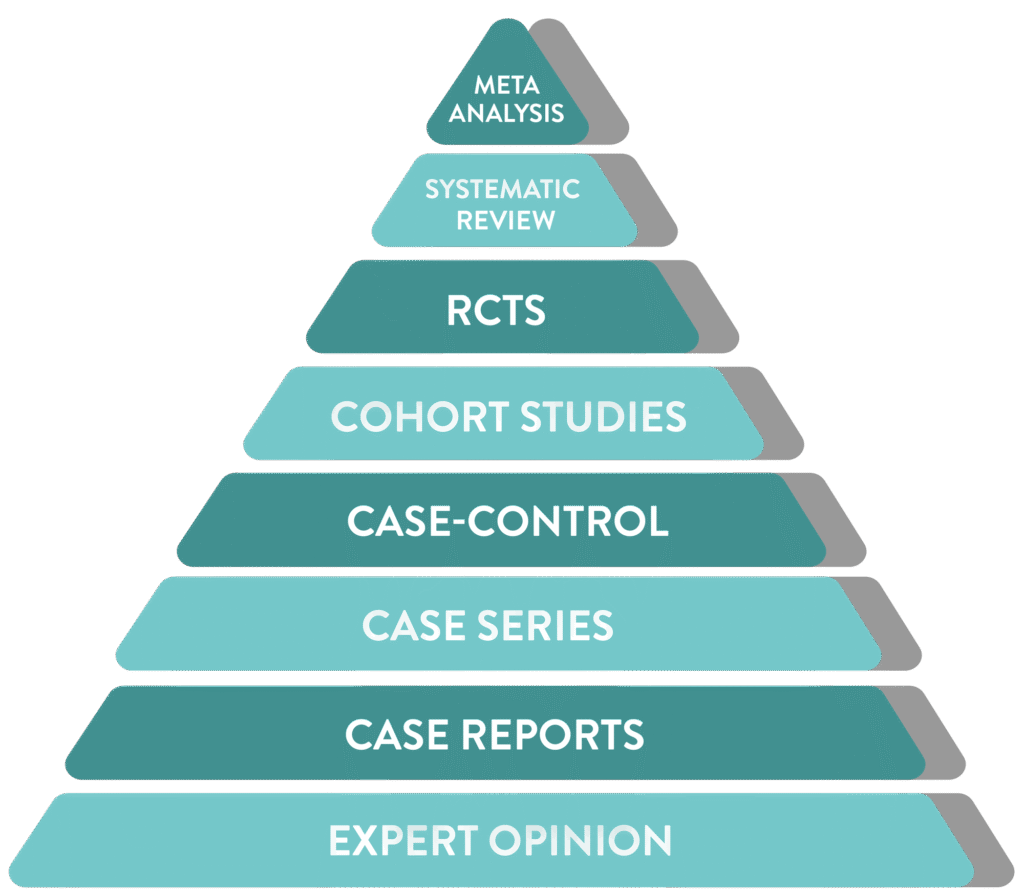

Incorporation of all available data with non-critical bias
Meta
Analysis
Analysis
Statistically combines data from multiple studies
Systematic
Review
Review
Summarizes all relevant studies on a topic
RCTs
Randomized trial comparing interventions, often to a control or placebo group
Cohort Studies
Follows groups over time to assess outcomes
Case-Control
Compares patients with a condition to those without
Case Series
Summary of similar cases in multiple patients
Case Reports
Detailed report on a single patient
Expert Opinion
Insights based on clinical experience rather than research
Henry et al. 2025 ![]() analysis of data until 20213
analysis of data until 20213
Hover your mouse over the pyramid to explore the hierarchy of scientific evidence.
